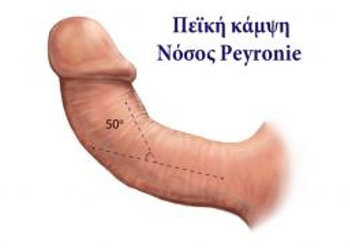
 Peyronie's disease is a relatively rare condition of the penis. Characteristic of the disease is the formation of a fibrous plate under the skin as a bump in the penis, resulting in the bending of the penis and pain during erection. Deformation and penile pain can make intercourse difficult or even impossible, disturbing the sexual and emotional relationship of the couple and negatively affecting the psychology and self-esteem of the man. This is a localized disease of the connective tissue in the fibrous envelope of the penis, which is the elastic housing of the penis' erectile infrastructure (i.e. the cavernous body). It is clearly a benign condition that occurs most often after the age of 45 and with increasing frequency as the man grows older, sometimes even occurring during a younger age. The disease occurs in 1-3% of the male population, but it is believed that this figure is much higher because of the reluctance of many patients to report their problem and seek help. The exact causes of the disease remain unclear and many opinions and theories have been expressed.
Peyronie's disease is a relatively rare condition of the penis. Characteristic of the disease is the formation of a fibrous plate under the skin as a bump in the penis, resulting in the bending of the penis and pain during erection. Deformation and penile pain can make intercourse difficult or even impossible, disturbing the sexual and emotional relationship of the couple and negatively affecting the psychology and self-esteem of the man. This is a localized disease of the connective tissue in the fibrous envelope of the penis, which is the elastic housing of the penis' erectile infrastructure (i.e. the cavernous body). It is clearly a benign condition that occurs most often after the age of 45 and with increasing frequency as the man grows older, sometimes even occurring during a younger age. The disease occurs in 1-3% of the male population, but it is believed that this figure is much higher because of the reluctance of many patients to report their problem and seek help. The exact causes of the disease remain unclear and many opinions and theories have been expressed.
Symptoms and course of the disease
The clinical picture of Peyronie's disease varies from person to person in terms of the number and severity of the symptoms and the rate at which the disease progresses. Symptoms include: palpable induration/plaque usually on the dorsal (upper) surface of the penis, without excluding its localization on other parts of the penis. Rarely, the plaques can be multiple. Usually bending and angulation of the penis are both present during erection. The deformation that occurs may be significant and there can be a shortening of the penis' length. There is also pain during erection and a reduced penis diameter.
It is estimated that 30% of patients with Peyronie's disease eventually suffer from erectile dysfunction due to the significant penile deformity that prevents proper penetration of the vagina. Erectile dysfunction may also be due to the malfunction that exists at a vascular level, but also because of the emotional and psychological problems resulting from the patient's disordered sexual life.
Spontaneous remission or complete cure of the disease occurs in 10-20% of patients. About 50% remain stable after the initial assessment, and in 30-40% of cases the disease worsens. Symptoms such as retention of the plaque for more than 12 months, calcification of the lesion and the presence of Dupuytren's disease (crinkling of palmar aponeurosis) are indications that eliminate the possibility of automatic improvement of the disease.
Treatment
Treatment of patients with Peyronie's disease during its early stages, should be as conservative as possible, taking always into account the seriousness of each individual case until the condition is stabilized and re-assessed. Patients should be encouraged to remain sexually active, as there is no data to show that sexual activity can exacerbate the situation.
Oral drugs include: Vitamin E, Colchicine, Tamoxifen, Acetyl-L-carnitine and Para-aminobenzoic potassium (Potaba). Also, local therapy drugs may be applied onto the lesion such as Verapamil, Collagenase, Steroids and Interferon-a2b
A time span longer than 12 months from the date of the diagnosis has to elapse in order for a surgical treatment to be considered and performed. Additionally, the fibrous plaque has to remain in a stable condition for 6-months, since there is always the possibility of automatic improvement during that period. Surgical treatment of Peyronie's disease is indicated if conservative treatment fails and deformation of the penis is so severe that makes contact difficult or impossible. The goal of the treatment is simply to make both sides of the penis equal. The amount of bending, the size of the plaque and the quality of the erection/degree of erectile dysfunction, determine the therapeutic technique that is eventually applied.
The principal surgical techniques are as follows: Removal of the plaque and implant insertion. Removing part of the fibrous envelope of the penis and implant insertion (thus avoiding complications arising from removing only the fibrous plate).
Creasing of the cavernous body of the penis where the plaque is not removed. Placing an insert inside the penis (in case of a co-existing severe erectile dysfunction due to the high degree of venous leakage).